

Prostate cancer screening around the globe
Fascinating perspective on how many countries are considering policy changes

Howard Wolinsky, who publishes the excellent The Active Surveillor newsletter, wrote recently, “Recommendations on PSA screening (for prostate cancer) are all over the map - literally all over the map.”

You can read more about how Australia, Great Britain, Lithuania, and Canada are considering changes in national policy for prostate cancer screening and the PSA blood test - with the Netherlands, Portugal, Croatia, Czech Republic, and parts of Spain watching data from other countries before making any changes.
Wolinsky knows this topic very well - as a longtime journalist and because he’s been diagnosed with prostate cancer, with a strong international following for his newsletter (2,500 readers from 76 countries). He reminds us:
PSA screening is such a tricky topic because the test used for screening is so unreliable. A British panel just said widespread screening would result in widespread overdiagnosis and overtreatment, resulting in balance greater harm. British patient advocates strongly disagree. This goes on, and on, the world go round.
Here is his article on the UK recommendation.

Two months ago, the massive European Randomized Study of Screening for Prostate Cancer published its 23-year results.

It has followed 162-thousand men ages 55-69 from eight European countries. It concluded:
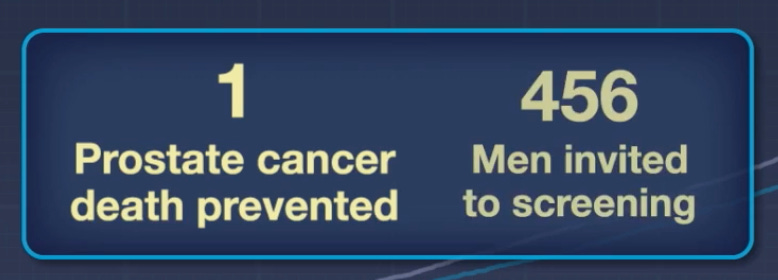
Long-term follow-up confirms a sustained reduction in deaths from prostate cancer with PSA testing, alongside an improved harm–benefit ratio. Future screening strategies should adopt risk-based approaches to minimize overdiagnosis while maintaining clinical benefits.
This may be the easiest statistic for most readers to grasp - 456 men would need to be screened in order to prevent one death.
Dr. John Mandrola, a cardiac electrophysiologist, published his reactions to the results on his Substack newsletter.
He explains that, as a patient, he initially refused a PSA blood test “but in a recent moment of weakness gave in.” Now, though, he writes that the results of the big European study “reinforce my initial opposition to being screened with a PSA test.” He wrote:
The absolute rates of prostate cancer deaths were 1.4% vs 1.6% in the screened vs control arm. So the absolute risk reduction was 0.2%. This means that the number needed to screen to prevent one prostate cancer death is approximately 500. I like to think of this as: 499 out of 500 men get no benefit from being invited to be screened.
In short, he views this as “a minimal absolute risk reduction in prostate cancer deaths (0.2%), no difference in overall mortality, and we know that there are potential complications from biopsies and surgeries.”
He acknowledges that urologists may view this quite differently. He wraps up:
I can only speak from the Neutral Martian and patient perspective.
Namely, that having a positive PSA would be a buzzkill. You would worry about it. You would have to go to for MRIs, genetic tests, etc. Maybe you could avoid a biopsy. Maybe not.
In the absence of better effect sizes on reduction of mortality, my minimizer-brain, sees the 9,999 other diseases that could take me out. And I would pass on PSA screening.
A maximizer brain might think otherwise, and that is fine. But I would hope doctors discuss this data with their patients. And would be humble about how much we can “prevent” bad outcomes in people without complaints.
He got 151 reader comments in response to his reactions - many in agreement, some not. Which is another glimpse of why Howard Wolinsky says “recommendations on PSA screening are all over the map.” Wolinsky wrote about the big study results, with this headline:

Screening discusssions never adequately value the downside of not testing.
In the case of PSA tests in the USA, the adverse USPSTF recommendations in 2012, 2016 and 2018 are now clearly reflected in the numbers. +/- 1 in 5 men diagnosed with prostate cancer are de novo metastatic. That's around 4 times the number who were first diagnosed metastatic 15 years ago.
We see a significant uptrend in prostate cancer specific mortality that many of us advocates predicted back in 2012. This may be the first year where ACS forecast diagnoses exceed breast cancer, and maybe deaths too.
By not testing, these advisories consign many more men to an early grave. I was a casualty of not testing, but fortunately had a diligent urologist or would not be writing this today.
Critics of PSA testing fail to understand that PSA testing is not responsible for overtreatment. Poor medicine and physician practices causes that. PSA testing is about information, not treatment.
Excellent piece, Gary!